Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy/Ablation
The medical procedures known as lumbar, cervical, or thoracic radiofrequency neurotomy (RFN) or denervation aims to alleviate neck, upper back, or lower back and/or leg/ arm pain stemming from facet joint issues. RFN is also referred to by various terms such as radiofrequency ablation, denervation, lesioning, rhizolysis, or rhizotomy, all describing the same procedure.
Radiofrequency neurotomy employs radio waves to generate heat, reaching about 85°C, which is then targeted via a thin needle to a specific nerve tissue area. While not completely destroying the nerve, RFN disrupts its ability to transmit pain signals to the spinal cord and brain, often providing longer-term pain relief compared to other injectable treatments.
Before undergoing RFN or radiofrequency denervation, patients typically receive a diagnostic nerve block (called a medial branch block) to ascertain if the specific nerve is indeed responsible for the pain. If the nerve block significantly and temporarily reduces pain, a neurotomy may be recommended as a more enduring solution.
Post-procedure, nerve tissue regeneration occurs gradually over 6 months to 2 years. If pain returns, which may not always be the case, repeat neurotomy might be necessary. Many patients who undergo lumbar, cervical, or thoracic RFN report pain relief lasting a year or more.
Table of Contents
- What is Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy?
- What Does Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy Address?
- How Does Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy Alleviate Chronic Neck and Back Pain?
- Why Would You Get Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy Treatment for Chronic Pain?
- Risks of Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy
- The Process of Getting Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy
- Preparing for Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy
- After Getting Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy (Follow-Up)
- Finding a Doctor Who Performs Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy Near You
- Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy at Persistent Pain Solutions
What is Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy?
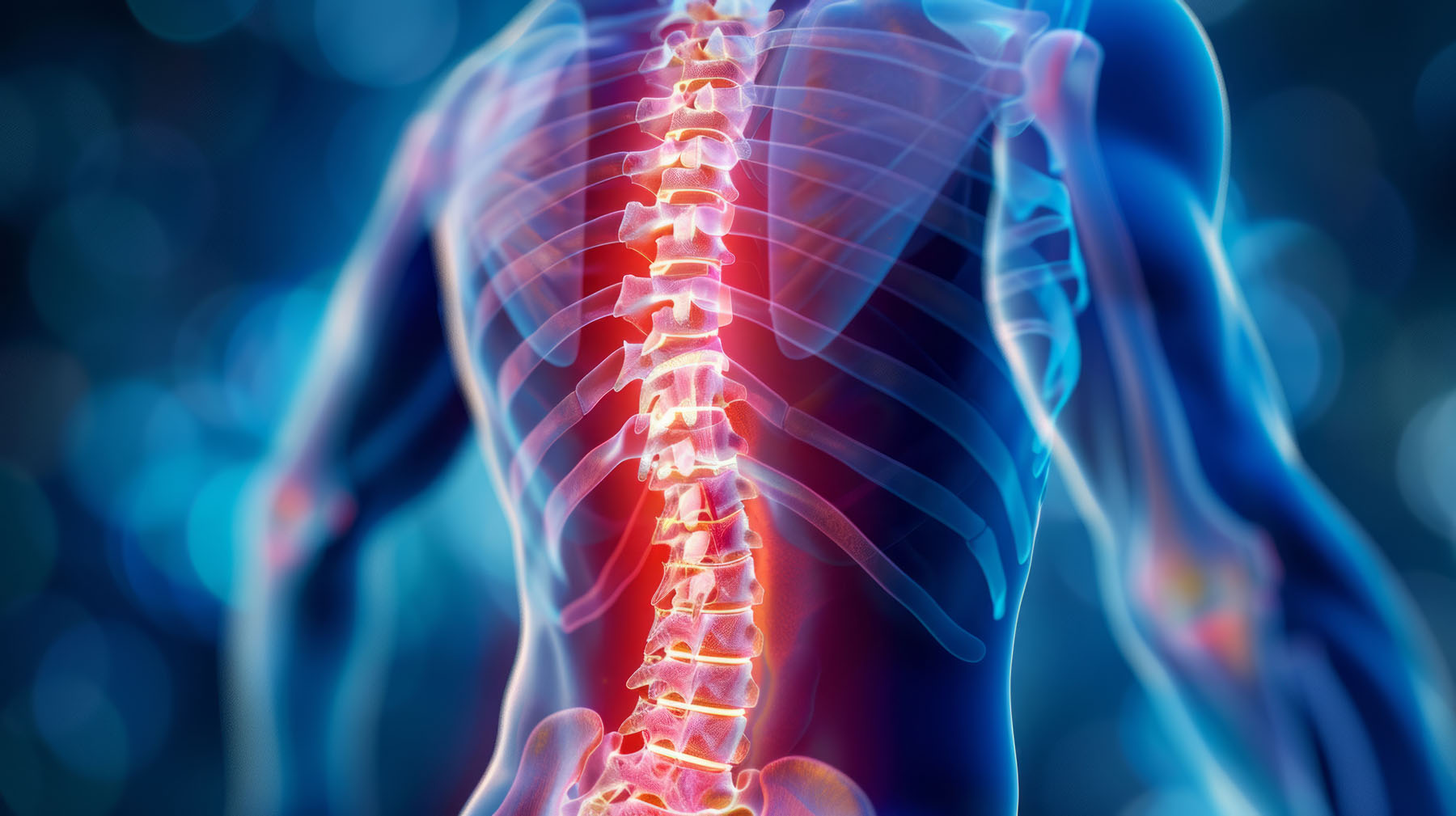
Lumbar, cervical, and thoracic medial branch radiofrequency denervation, also known as neurotomy, is a minimally invasive procedure used to alleviate chronic pain originating from the facet joints in the spine. Facet joints are small joints located between each vertebra, and they can become a source of pain due to conditions such as arthritis, injury, or degeneration.
During the procedure, radiofrequency energy is used to target and disrupt the function of the medial branch nerves that supply sensation to these facet joints.
The process involves placing a specialised needle with an electrode tip near the targeted nerves under fluoroscopic (X-ray) guidance. Once the needle is correctly positioned, radiofrequency energy is delivered through the electrode, generating heat that creates a lesion on the nerve. This interrupts the nerve’s ability to transmit pain signals to the brain, providing relief for the patient.
Lumbar, cervical, and thoracic medial branch radiofrequency denervation procedures are primarily used for individuals who have undergone prior diagnostic medial branch blocks and have experienced significant pain relief from these blocks. The goal of radiofrequency neurotomy or denervation is to provide longer-lasting pain relief compared to temporary blocks or other conservative treatments.
It is important to note that while radiofrequency denervation can provide effective pain relief for many individuals, the duration of relief can vary from person to person. Some patients may experience relief for several months to a year or more, while others may require repeat procedures over time. Generally speaking, RFN of the medial branch nerves can reduce pain by 50-80%, lasting for 12-18 months. The procedure can take up to 6-8 weeks to achieve maximal benefit. There is a good probability of success of RFN if the patient has had a positive diagnostic medial branch block, but it is important to note that success cannot be guaranteed due to the effects of placebo which occurs in around 30% of patients undergoing a medial branch block.
Additionally, the procedure carries potential risks and complications, which should be discussed with your doctor before undergoing the treatment.
What Does Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy Address?
Lumbar, cervical, and thoracic medial branch radiofrequency denervation, also known as neurotomy, is used to treat chronic pain originating from the facet joints in the respective regions of the spine.
- Lumbar Region (Lower Back). This procedure is employed to address chronic lower back pain stemming from facet joint dysfunction in the lumbar spine. Facet joint issues in this area can result from conditions such as arthritis, injury, or degeneration, leading to persistent discomfort or stiffness in the lower back. Occasionally the pain from facet joint dysfunction can radiate into the buttocks and the legs.
- Cervical Region (Neck). In the cervical spine, radiofrequency neurotomy targets chronic neck pain arising from facet joint problems. Individuals experiencing cervical facet joint dysfunction may suffer from neck stiffness, limited range of motion, and radiating pain into the shoulders or arms.
- Thoracic Region (Mid-Back). Radiofrequency denervation can also be utilised to alleviate chronic pain in the thoracic spine caused by facet joint issues. Pain in the thoracic region may manifest as discomfort between the shoulder blades, stiffness, or pain that radiates around the rib cage.
How Does Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy Alleviate Chronic Neck and Back Pain?
Lumbar, cervical, and thoracic medial branch radiofrequency denervation or neurotomy alleviates chronic neck and back pain by targeting the nerves responsible for transmitting pain signals from the facet joints in the spine.
Here is how it works:
- Targeted Nerve Ablation. During the procedure, a specialised needle with an electrode tip is precisely positioned near the targeted medial branch nerves under fluoroscopic (X-ray) guidance. Radiofrequency energy is then delivered through the electrode, generating heat that creates a lesion on the nerve. This targeted ablation disrupts the nerve’s ability to transmit pain signals from the facet joints to the brain.
- Pain Signal Interruption. By creating lesions on the medial branch nerves, radiofrequency neurotomy interrupts the transmission of pain signals. This effectively reduces or eliminates the sensation of pain originating from the facet joints in the lumbar, cervical, or thoracic regions of the spine.
- Longer-Term Pain Relief. Unlike temporary treatments such as nerve blocks or corticosteroid injections, radiofrequency denervation provides longer-lasting pain relief. By disrupting the function of the nerves responsible for transmitting pain signals, the procedure can provide relief for several months to a year or more for many individuals.
- Improved Function and Quality of Life. By alleviating chronic neck and back pain, radiofrequency neurotomy can improve mobility, reduce stiffness, and enhance overall quality of life for individuals suffering from facet joint dysfunction in the lumbar, cervical, or thoracic spine.
Lumbar, cervical, and thoracic medial branch radiofrequency neurotomy or denervation procedures offer an effective and minimally invasive treatment option for chronic neck and back pain, providing long-lasting relief and improving one’s ability to perform daily activities.
Why Would You Get Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy Treatment for Chronic Pain?
You may consider lumbar, cervical, and thoracic medial branch radiofrequency denervation (or neurotomy) treatment for chronic pain if you have been diagnosed with facet joint dysfunction in the respective regions of your spine and have not found adequate relief from conservative treatments such as medication, physical therapy, or injections.
Here are some reasons why you might opt for this treatment:
- Persistent Pain. If you experience chronic neck or back pain that significantly impacts your daily activities, despite trying other non-invasive treatments, radiofrequency neurotomy may offer longer-lasting relief by targeting the nerves responsible for transmitting pain signals from the facet joints.
- Diagnostic Confirmation. Prior to undergoing radiofrequency denervation, patients typically undergo diagnostic medial branch blocks to confirm that the facet joints are indeed the source of their pain. If you experience significant pain relief from these blocks, radiofrequency neurotomy may be recommended as a more enduring treatment option.
- Longer-Term Relief. Unlike temporary treatments such as nerve blocks or corticosteroid injections, radiofrequency denervation provides longer-lasting pain relief by disrupting the function of the nerves transmitting pain signals. This can improve your quality of life and allow you to engage in daily activities with reduced discomfort for several months to a year or more.
- Reduced Need for Medications. By addressing the root cause of your pain, radiofrequency neurotomy may reduce your reliance on pain medications, which can have potential side effects and limitations in managing chronic pain over the long term.
- Improved Functionality. Alleviating chronic neck or back pain with radiofrequency denervation can improve your mobility, reduce stiffness, and enhance overall functionality, allowing you to participate more fully in activities of daily living and potentially return to work or recreational activities that were previously limited by pain.
Risks of Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy
While lumbar, cervical, and thoracic medial branch radiofrequency denervation (neurotomy) is generally considered safe, like any medical procedure, it carries certain risks and potential complications. Some of the risks associated with this procedure include:
- Injection Site Reactions. Some patients may experience temporary pain, discomfort, or bruising at the injection site.
- Flare up of pain. There may be a temporary flare up of pain which can last for up to 1-2 weeks after the procedure. This is often related to inflammation at the injection site or temporary irritation of the nerves. You will be provided with analgesia after the procedure to assist with this flare up of pain.
- Infection. There is a risk of infection at the injection site, although this is rare. Signs of infection include increased pain, swelling, redness, or drainage from the injection site.
- Bleeding. There is a risk of bleeding at the injection site, especially for patients taking blood-thinning medications. This can lead to hematoma (collection of blood) at the injection site.
- Allergic Reactions. Allergic reactions to the medications used in the injection, such as local anaesthetics or corticosteroids are possible but uncommon. If a contrast dye is used during the procedure, there’s a slight risk of an allergic reaction to the dye, which may include rash, itching, or more severe reactions like anaphylaxis.
- Hypersensitivity/ Numbness. You may experience an area of increased sensitivity or numbness in the region of the procedure. This is usually temporary and resolves within 6-8 weeks.
- Nerve Damage. Although rare, there is a small risk of nerve damage due to needle placement (direct trauma), the medication injected, infection or bleeding. Symptoms may include numbness, tingling, weakness, or increased pain or neurological symptoms.
- Spinal Cord or Nerve Root Injury. Although extremely rare, there is a risk of injury to the spinal cord or nerve roots during the injection, which can lead to neurological deficits, bowel and bladder dysfunction, numbness and paralysis. .
- Exposure to X-Rays and CT. Minimal doses of radiation are used to reduce the lifetime risk of long term complications (such as cancer) due to exposure to X Ray and/ or CT scanning.
- Incomplete Pain Relief/ Failure. While many patients experience significant pain relief following radiofrequency denervation, the procedure may not provide complete relief for everyone. Factors such as individual pain tolerance, underlying conditions, or nerve regeneration over time can affect the outcome. Hence, the procedure may not provide the expected result or benefit.
- Sedation anaesthesia. There are risks of undergoing the sedation anaesthetic which is discussed on the day by the anaesthetist. Anaesthesia is generally very safe but there may be increased risk depending on your specific medical conditions.
It is essential to discuss the potential risks and benefits of lumbar, cervical, or thoracic medial branch radiofrequency denervation with your physician before undergoing the procedure. Additionally, these procedures must be performed by trained and experienced healthcare professionals in a controlled medical setting to minimise risks and ensure your safety.
The Process of Getting Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy
The process of getting lumbar, cervical, and thoracic medial branch radiofrequency denervation or neurotomy typically involves several steps:
- Consultation. The process often begins with a consultation with a pain management specialist or anaesthetist. During this consultation, the healthcare provider will review the patient’s medical history, perform a physical examination, and discuss the nature and location of the pain.
- Diagnostic Evaluation. Based on your symptoms and medical history, the healthcare provider may order diagnostic tests such as X-rays, MRI, CT scans or CT spect bone scans to evaluate the spine and identify any potential sources of pain, such as facet joint dysfunction.
- Informed Consent. Before the procedure, your doctor will explain the risks, benefits, and alternatives of lumbar, cervical, or thoracic medial branch radiofrequency denervation. You will have an opportunity to ask questions and provide informed consent for the procedure.
- Preparation. On the day of the procedure, you will be asked to refrain from eating or drinking for a certain period before the appointment, depending on your doctor’s instructions. You will also be asked to change into a hospital gown. The procedure is performed under sedation anaesthesia to prevent discomfort during the procedure.
- Procedure. You will be positioned on an examination table, either lying face down (prone). The skin over the injection site(s) will be cleansed with an antiseptic solution.
- Local Anaesthesia. The specialist will use a local anaesthetic to numb the skin and underlying tissues at the injection site(s). This helps minimise discomfort during the procedure.
- Needle Placement. Using fluoroscopy (X-ray) guidance, your doctor will carefully insert a specialised needle with an electrode tip near the targeted medial branch nerves that supply sensation to the facet joints. Once the needle is in the correct position, radiofrequency energy will be delivered through the electrode to create lesions on the nerves.
- Post-Procedure Monitoring. After the procedure, you may be monitored in the recovery area to ensure there are no immediate complications. You will be instructed to log your pain levels and any changes in symptoms on a Pain Chart over the following 6 weeks.
- Follow-Up. Depending on the individual response to the procedure, your doctor may schedule a follow-up appointment to assess the effectiveness of the radiofrequency denervation in alleviating pain and to discuss further treatment options if needed.
Overall, the process of getting lumbar, cervical, or thoracic medial branch radiofrequency denervation involves careful preparation, precise needle placement, and post-procedure monitoring to ensure patient safety and optimise outcomes.
Preparing for Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy
Preparing for a lumbar, thoracic, or cervical medial branch radiofrequency denervation at the Persistent Pain Solutions clinic will require close communication with Dr Mittal and her team.
Be sure to disclose all medications you may be taking and note that you may have to discontinue some or all of them immediately prior to the procedure.
Prior to your appointment, please inform us if:
- You are currently taking antibiotics.
- You have a pacemaker or defibrillator.
- You have any allergies.
- You have diabetes.
- You are taking any blood thinning medications.
- You are feeling unwell, as we may need to reschedule your procedure.
You must also avoid eating or drinking anything in the six hours leading up to the procedure. However, you may continue to take medications with a small sip of water on the morning of the procedure. You will be advised to cease some other medications such as those for diabetes and blood thinning medications.
For your safety, we recommend arranging transportation to and from your appointment, as driving yourself is not advised within the 24-hour period following the procedure.
We generally recommend you take leave from work on the day of the procedure AND for 1 – 2 weeks after the procedure, to rest and recover from the procedure.
If you are receiving medial branch radiofrequency denervation, we advise you to refrain from undergoing any additional medical procedures, such as dental treatments or colonoscopies, within 48 hours before or after undergoing the medial branch radiofrequency denervation procedure.
Dr Meena Mittal and her team will provide specific guidance tailored to your situation. It’s important to adhere to your instructions diligently. If you have any concerns or queries, don’t hesitate to ask—we’re here to support you throughout the process.
After Getting Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy (Follow-Up)
Following your medial branch radiofrequency denervation procedure, you are free to return home.
There are no specific restrictions on your day-to-day activities. However, it is advisable to prioritise rest and engage in gentle activities during the initial 24-48 hours after your procedure. Due to sedation administered during the treatment, please refrain from driving for at least 24 hours afterwards.
You may commence physiotherapy 2-4 weeks after the procedure. You may return to hydrotherapy or a swimming pool/ spa 2-4 weeks after the procedure.
We do not recommend any long distance or overseas travel for at least 2-4 weeks after the procedure. This is such that any issues or complications can be monitored and addressed in a timely manner.
A follow-up appointment will be scheduled at 6 weeks post procedure to assess your response to the radiofrequency denervation procedure. You will be requested to bring the post procedure Pain Chart such that the results can be analysed by Dr Mittal and next steps in your treatment plan can be discussed with you.
Finding a Doctor Who Performs Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy Near You
If you are suffering from chronic neck pain, upper back pain, or lower back pain, then a pain specialist who offers lumbar, cervical, or thoracic RFN may be able to provide relief.
Seek a referral from your general practitioner for a pain management doctor who offers lumbar, cervical, or thoracic medial branch radiofrequency neurotomy or similar procedures for neck and back pain. You can also research pain management clinics online or speak to family members, friends, or (online or real life) support groups for recommendations from others dealing with chronic back or neck pain.
Lumbar, Cervical, and Thoracic Medial Branch Radiofrequency Denervation/Neurotomy at Persistent Pain Solutions
The Persistent Pain Solutions clinic provides lumbar, cervical, and thoracic medial branch radiofrequency denervation or neurotomy. These procedures help alleviate neck and back pain by targeting the medial branch nerves in the facet joints that run along the length of your spine.
Thoracic, cervical, and lumbar medial branch radiofrequency denervation or neurotomy can significantly alleviate back and neck pain, improving your overall quality of life.

Find a Persistent Pain Solutions Location Near You
Leader in Personalised Care, Integrative Pain Medicine, & Pain Management Intervention.
Pain Treatments We Offer in Melbourne, Victoria
Don’t Miss an Update
Join our newsletter to learn more about our staff, patients, and communities in the know on all of the recent news, events, and announcements for Persistent Pain Solutions.